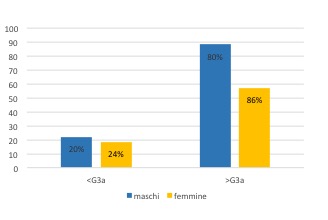
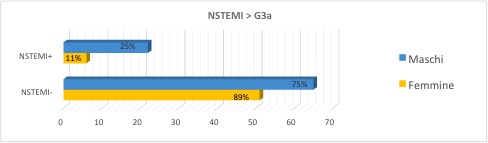
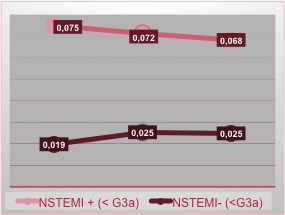
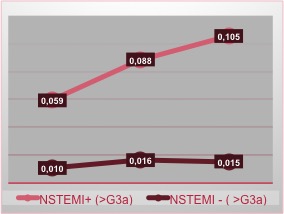
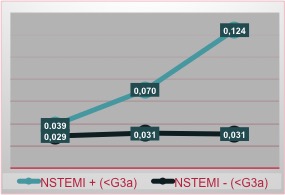
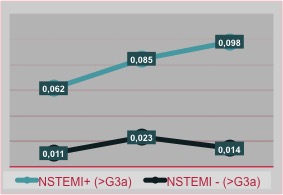
In light of the results obtained, we can assess a greater prevalence of NSTEMI in the male CRF+ sample compared to the female. In males, the canonical but steep pattern of the curve suggests us to carry out the third measurement to avoid missing diagnosis. In women, however, the flat trend suggests the need to use additional diagnostic pathways because the troponins alone may not be sufficient, even if the value is higher than the norm, but does not describe a peak.
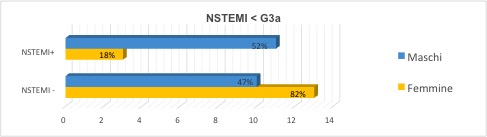
The basal value (T0) of troponins in CRF+ and NSTEMI- patients differs considerably from the value of CRF- patients, which leads us to hypothesize that in CRF+ patients there is a chronic rise in the values of troponin not related to ACS. That’s why we could “suggest” the troponin value 0,024 μg/L*, common to both genders, as an useful item to use in emergency setting, when we face patients with CRF (<G3a stage). However, it is very clear that it is necessary to enlarge the sample in order to improve the statistical power.
Limitations: the low numbers of the sample, also due to the subdivisions, requires to be increased, above all for the purpose of determining a special cut-off. The fragmentation operated to analyze gender differences and based on the renal function has inevitably decreased the statistical power.
Furthermore, what may have influenced the difference in the pattern of the curves, could be the time elapsed between the onset of chest pain and the T0 dosage of troponin: some patients, in fact, would have presented to ED very early and therefore the troponin levels could be still low. Other patients, on the other hand, would have presented late and therefore troponin levels could be already higher at T0.
*Relative to “Test Elecsys Roche” hs-cTnT tritation.